University of Rwanda’s College of Medicine and Health Sciences students have come up with an app called ‘Tantine App’, which will provide reproductive health education to young refugees and teens across the country.
The application which can be downloaded from Play Store was developed by Uhirwa Sylvie and Sylvain Hirwa Muzungu who are siblings. The duo is in their 5th year, pursuing Medicine.
The move also provides mentorship for young people especially girls with concerns about reproductive health using internet. It targets teens aged between 10 and 24. However, the developers added that other people who are above that age could benefit from the initiative especially pregnant women.
The app gives pregnant women chances to predict when they will deliver. It further gives useful pregnancy tips and info.
Uhirwa said that the android application is an opportunity for adolescents in refugee camps and outside as they will have a chance to interact, ask and get counseling from trained educators.
How the idea was conceived?
“My brother and I came up with an idea in 2015 when we were in year two. The initiative came as a result of trainings we had attended on sexual and reproductive health,” Uhirwa explained.
After a tour in Mahama refugees Camp, the young innovators realised that there was a need of more efforts to educate teens on reproductive health due to the experience they had gotten from the camp among adolescents.
“Besides our own experience, we also relied on the studies conducted on reproductive health among teens where unwanted pregnancies and HIV/AIDS were the issues of concern, she added.
“Most teens don’t have adequate knowledge on reproductive health. Therefore, we asked ourselves what we should do as students in health sector to help them,” Uhirwa said.
Tantine’s homepage. / Faustin Niyigena
The University of Rwanda students created a Facebook page which is currently followed by over 5,000 people to share information about reproductive health.
Later on, Tantine project was validated to compete in young innovators projects about reproductive health which was organized by Makerere University and fortunately the project was pitched and funded.
Winning iAccelerator contest
In February, the project competed in iAaccelerator, a mentorship-driven acceleration programme which aims to explore new and engaging ways to tackle pressing sexual and reproductive health challenges, while promoting social entrepreneurship among young people. It was pitched among top four projects and walked away with a grant of $10,000, to help develop their ideas into workable products.
“We competed with 200 hundreds projects and our project was selected among the top ten and finally pitched among four top winners and awarded,” she said.
Developing Tantine App
The grant helped the young innovators to think of how to develop their project to reach more beneficiaries.
“Due to the advancement of technology, we thought of how to come up with a new App to enable beneficiaries to access our services easily. That is the reason why we developed this application,” Uhirwa explained.
The new App was launched in August this year.
It has different parts from which beneficiaries get reliable information about reproductive health, provide ideas and comments as well as asking questions.
The Tantine App on the Google Play Store has far attracted a hundred users. / Faustin Niyigena
Future plans
The developers plan to conduct campaigns in different schools on reproductive health.
The e-Health project also intends to integrate the use of Tantine website (www.tantine.rw) and its application in the University of Rwanda so that students can get reliable reproductive health information and services. They also plan to expand the project to other refugee camps in Rwanda and beyond.
“We shall appoint Tantine ambassadors in various schools who will be sharing Tantine’s products with their peers,”
In order to sustain and develop the project, the developers have welcomed two more members to ensure the sustainable and success.
Marie-Claire Umuhoza, another stakeholder in charge of marketing, said that reading culture is still a big challenge among teens.
“We provide important information but the problem is that young people are weak in reading,”Umuhoza said.
At the beginning, young innovators faced a challenge of confidentiality where beneficiaries could not believe what they were serving.
Another challenge is insufficient financial support to ensure the sustainability and promote the products to all beneficiaries countrywide.
The group does not work alone because they are partnering with some medics who advise them and inspire.
Aspirations
The young innovators call for support from the Ministry of Health and Ministry of Youth to promote the App by raising awareness among teens because the developers believe the move will contribute much to the health sector.
People with extremely high levels of so-called “good cholesterol” have a 65% higher mortality rate than people with normal levels, according to a new Danish study. Does this mean that good cholesterol has gone from hero to villain? Can we still consider good cholesterol to be good?
Cholesterol, it seems, is never far from the news. Scientific studies frequently report that cholesterol, and the drugs that control cholesterol such as statins, are implicated in many diseases beyond heart disease, from Alzheimer’s disease to cancer. Cholesterol is essential for life, and is found throughout the body. It is a waxy substance made in the the liver but is also found in some foods, including full-cream dairy and animal fats.
Cholesterol can’t travel through the blood on its own as it doesn’t dissolve in the watery blood plasma. In order to travel in the blood, cholesterol combines with proteins to form lipoproteins. There are two main types of lipoproteins, low-density lipoproteins (LDL) and high-density lipoproteins (HDL). LDL is commonly referred to as “bad cholesterol” because it delivers cholesterol from the liver to the other cells in the body. HDL is known as “good cholesterol” as it does the reverse, carrying cholesterol back to the liver to be broken down.
In the new Danish study, over 116,000 Danish men and women were pooled together from two large study cohorts. Participants had a blood sample taken at the start of the study, where their cholesterol was measured. They were then followed up for a number of years – in some cases, for as long as 23 years.
During the follow-up period, over 10,000 participants died. When the researchers analysed the data, they found something very interesting. The relationship between HDL levels and mortality was U-shaped. This means that people with either extremely high or low concentrations of HDL had an increased risk of death. This means that those people with the highest levels of HDL were more likely to die than those with normal levels of HDL, and about as likely as those with the very lowest levels of HDL.
There were some noticeable differences between men and women, with the ideal HDL level in men being around 25% lower than in women.
The researchers might have anticipated that low levels of HDL would be a risk factor for an early death, but evidence that the highest levels of HDL carry a similar risk is very interesting. So what do these findings mean for the rest us?
A genetic cause?
No study is perfect, and although this study was very large it relied on a single blood sample at the point of recruitment, and was limited to white people of Danish descent. This means that any changes in HDL level that may have occurred throughout the study were not taken into account, and that the findings may not be applicable to more ethnically mixed populations.
Very few people actually have very high HDL levels, and in this study only 216 men and 218 women out of 116,000 showed the highest concentrations of HDL, so the number of people affected in real terms may be low, even if the relative risk is high.
The study does, however, give us an opportunity to consider what we really know about HDL. Although consistent observational evidence of the relationship between HDL and heart disease risk exists, the relationship doesn’t appear to be causal as boosting HDL levels (but not to ultra-high levels) using drugs doesn’t decrease the risk of heart disease or early death.
It is possible that a genetic mutation is the root cause of extremely high HDL, which is why these cases are so rare. As HDL has subtypes, it is also possible that one or more of these subtypes are key in preventing heart disease, but more research is needed to confirm this.
Doctors should take note of this study and consider that if they see cases of extremely high levels of HDL in their patients it may be worth monitoring. It is, however, unlikely that many people reading this article will have HDL levels high enough to cause them, or their doctor, to worry. In general, it is still a good idea to assume that good cholesterol is good for your heart.
Vinyl records and cassette tapes, the parties that went with them, and other hedonistic pleasures from our youth can form a big part of our identity years later. from www.shutterstock.com
Are the hedonistic adventures of your late teens and 20s fresh in your memory? Can you easily recall footloose years when school ended and before serious adult life began? Perhaps you enjoyed a few years of partying until dawn, nights of cheap wine, good friends and song. Or maybe it was all so wild that you remember nothing at all.
Bruce Springsteen sang about looking back on these “glory days”; the days before careers, children or other responsibilities took over.
Bruce Springsteen’s Glory Days captures the days before careers, children or other responsibilities took over.
Of course, not everybody has time or the opportunity to party, or remembers their youth with perfect pleasure. But why do many of us still recall so vividly and tell stories of our hedonistic younger days? Why do such memories remain rosy and important touchstones?
Memory is selective
The first reason is that memory is selective. To remember an experience or event we need to pay attention to it. Then we need to rehearse it by thinking or talking about it. Events that are “encoded” in this way are “stored” in our long-term memory.
But not everything we do, say or feel everyday is encoded and stored in memory. We are more likely to encode events that stand out, are highly emotional, mark first-time experiences or represent big changes in our lives: your first ever muddy music festival or a party that got wonderfully out of control.
“Hold onto 16 as long as you can” – John Mellencamp, Jack and Diane.
Recalling or “retrieving” events from our long-term memory also is motivated. By motivated we mean that remembering some events but not others serves a psychological purpose. We tend to remember events from the past that are consistent with how we want to see ourselves now. Our sense of identity and memories are completely intertwined.
Former party animals thinking about their past selectively remember party animal memories. Each time they think of these memories, instead of memories inconsistent with this picture, they reinforce a particular view of themselves and their hedonistic past.
Memory researchers call this “retrieval induced forgetting”: by repeatedly rehearsing or practising some memories (“that time I partied all night”), we forget about other related memories (“that time I studied all night”), shaping and reshaping our sense of the past and ourselves.
Memories of our teenage years matter
The second reason is a phenomenon known as “the reminiscence bump”. When we look back over the past, we don’t remember an equal number of events across our lives. Instead, we remember more from our teenage and early adult years.
Memories in this reminiscence bump overwhelmingly are of positive, not negative, experiences. Researchers have long speculated why, but one explanation is these are the years when we form a stable lifelong identity.
Because the events that happen to us in this “bump” are formative and central to how we view ourselves, we tend to remember them well. And because – for most of us – we selectively remember the past to form a positive, optimistic identity, we encode and store positive rather than negative memories.
“Those were the best days of my life” – Bryan Adams, Summer of ‘69.
Interestingly, the reminiscence bump applies not just to our personal experiences, but also to the music we recognise and love. This personally significant music usually dates from our teenage and early adult years and can trigger vivid memories decades later.
So the identity we form in our early adulthood – the wild child – shapes our recollections and helps shape us for the rest of our lives – the former wild child settling down.
Memory can be a social glue
The third reason is that memory is inherently social. We use memory to build our individual identity, but just as importantly, we use memory to build social bonds, entertain others and teach the next generation (“do what I say, not what I did”).
In fact, researchers have shown that adolescents who can re-tell their parents’ teenage memories and connect them to their own developing sense of identity report higher levels of psychological well-being.
“A long, long time ago, I can still remember …” – Don McLean, American Pie.
Over time, the exact details of what happened when we were young may become less important than the sense of belonging and shared identity we gain from joint reminiscing and storytelling.
Events become exaggerated, parties become wilder and bands become more amazing as we tell and re-tell stories for different audiences and different purposes: from nostalgic reminiscing at our high school reunion, to introducing our children to Pink Floyd, or starting those tricky parenting conversations about sex, drugs and rock ‘n’ roll.
So we remember and tell stories of our hedonistic past because these events were memorable, unless it was the 60s and you remember nothing! Remembering them also helps us to see ourselves then and now in desirable ways, and sharing these memories binds us to others in important ways.
But were we as wild as we remember? Perhaps or perhaps not. But our memories of more carefree times serve us well.
Read other articles in our hedonism and health series:
Hedonism and pleasure is what drives much binge drinking. So let’s provide people with alternative ways of having fun, but without the alcohol. from www.shutterstock.com
This is the second article in our three-part series on hedonism and health. Today, we look at the complex relationship between hedonism and binge drinking – part cause, part solution.
Hedonism – the pursuit of pleasure, enjoyment, or fun – might sound like a strange way to tackle binge drinking. After all, we usually associate hedonism with triggering binge drinking in the first place.
Binge drinking with other people increases pleasure so drinking with friends is more pleasurable than drinking alone. Drinking in a group can make people feel euphoric, a very enjoyable feeling.
I think people start drinking on a night out to “lubricate” conversation and to make them feel more relaxed. It takes away nerves of talking to the opposite sex and helps to lose inhibitions about dancing, singing, etc. It also helps people forget about current stresses in their life – none of these seem to matter when you’re drunk. So it serves as escapism from the daily grind.
Binge drinking can also increase the overall social experience by providing stories to tell friends (or to post on social media) afterwards.
While alcohol isn’t seen as a necessary part of a social occasion, it can enhance pleasure through social connectedness and intimacy.
People also drink to get drunk on purpose as a form of “calculated hedonism”. This helps people chill out or de-stress after a difficult week of work or study. And in an example of how people can moderate their hedonism, if people have a commitment the day after a night out, they are less likely to binge drink.
Using hedonism to tackle binge drinking
So, if hedonism motivates binge drinking what else could also provide this hedonistic benefit? What alternatives could we provide to meet the hedonistic needs of social connectedness, relaxation and happiness?
That’s where the field of social marketing comes in. Social marketing uses familiar marketing concepts (traditionally used, for instance, to market consumer goods) to improve social problems.
Traditional marketing sells alcohol. But social marketing can make it easier and desirable for people to drink responsibly, or to abstain. from www.shutterstock.com
There have been several successful examples of campaigns or strategies that have met people’s hedonistic needs, but without drinking.
The SUB21 campaign in the UK designs activities for young people such as nail art, bicycle repairs and BMX bike riding to come together and recreate that “Friday feeling” without drinking. This campaign reduced binge drinking levels, public drinking and alcohol purchases over a 12 month period.
Playing a game online or on your phone stimulates the pleasure centre of the brain and provides hedonistic benefits through the release of the happy hormones (dopamine and serotonin).
So, designing a game that not only provides hedonistic benefits, but also needs low or no alcohol levels to succeed can promote behaviour change.
For instance, social marketers developed a game called Risky Ride for high-school students to demonstrate the effects of drinking on physical ability and control. This reduced their intentions to binge drink.
Then there are campaigns that tap into the fact that alcohol reduces inhibitions and allows people to have fun because they don’t care what people think. Creating a non-judgemental environment can do the same.
For instance, the No Lights No Lycra dance community uses dim lighting and unpretentious venues to allow people to express themselves through dance.
The No Lights No Lycra movement provides opportunities for letting yourself go, but without the alcohol or the self-consciousness.
And the Hello Sunday Morning program has online and social media channels to help people share moderate drinking experiences with friends.
So hedonism can not only fuel binge drinking, by providing alternative pathways to pleasure, it can also help tackle the problem. Social marketing can work alongside alcohol regulation, policy and health promotion advertising to look for innovative ways of meeting hedonistic needs with reduced or no alcohol.
Business and social enterprise can also get involved as opportunities will arise for goods and services linked to these innovative ways of having fun without binge drinking.
Read other articles in our hedonism and health series:
Hedonism isn’t all about sex, drugs and rock ‘n’ roll. It can be about savouring the pleasure in a cup of tea at the end of a hard day. from www.shutterstock.com
This is the first article in our three-part series looking at hedonism and health. Today we look at what hedonism is (and is not), how it’s linked to your health, and how you can add (and appreciate) some simple pleasures in your daily life.
I think I might be a hedonist. Are you imagining me snorting cocaine through $100 notes, a glass of champagne in one hand, the other fondling a stranger’s firm thigh? Before you judge me harshly, I know hedonism has a bad reputation, but it might be time to reconsider.
What if, instead of a guaranteed one-way road to ruin, hedonism is good for your health? If we think of hedonism as the intentional savouring of simple pleasures – like playing in fallen leaves, moments of connection with friends, or cuddling the dog – then it probably is. Seeking and maximising these kinds of pleasures can boost our health and well-being.
So where do our ideas of hedonism come from and how can we harness hedonism to improve our health and quality of life?
The popular view of hedonism
In broad terms, a hedonist is someone who tries to maximise pleasure and minimise pain. Jordan Belfort (played by Leonardo DiCaprio) in The Wolf of Wall Street
is probably the popular idea of the quintessential hedonist, where his extreme wealth allows him to indulge his insatiable hunger for all things pleasurable.
Jordan Belfort (played by Leonardo DiCaprio) in The Wolf of Wall Street is one popular portrayal of a hedonist.
Hedonism Bot from Futurama is another character exquisitely in touch with things that provide pleasure.
Futurama’s Hedonism Bot knows what gives him pleasure, and it’s not always the usual suspects.
We find these characters so compelling because they seem to reject the sensible, responsible way to live. They indulge their carnal appetites in ways we daren’t, with scant regard for consequences. We wait for their liver to rebel or their life to come crashing down around them, as of course it must.
But this kind of behaviour is better termed debauchery – extreme indulgence in bodily pleasures and especially sexual pleasures – rather than hedonism.
Hedonism has its philosophical roots as far back as Plato and Socrates, but ancient Greek philosopher Epicurus is often credited with articulating an early brand of hedonism based not on a life of untamed appetites, but on moderate pleasures and respect for others.
It might help to think of pleasure simply as a subjective state of enjoyment. This is a broad perspective, but one easily applied to our everyday lives. So, a lover’s caress gives me pleasure, but so can a piece of music, laughing with friends, or simply sitting still in a comfy chair after a frantic day.
Just as different experiences can bring a similar shiver of pleasure, the same experience can conjure a range of responses — from extreme pleasure to definite displeasure — in different people.
There is no single stimulus that elicits exactly the same response in everyone all the time: pleasure is an interaction between the stimulus and the perceiver.
If you close your eyes and think about a time you experienced a tingle of pleasure, chances are you’re remembering a sexual experience, or something delicious you’ve eaten. Perhaps the memory is of a very good glass of wine, or those last 50 metres of a long, satisfying run.
And these are good things, right? Sexual pleasure is linked with health and well-being. For example, women who say they are satisfied with their sex life score higher on measures of psychological well-being and vitality. A regular glass of wine is said to have a protective effect against dementia and heart disease, perhaps due to its antioxidant flavonoids. And everyone knows the advantages of physical fitness.
Well, these activities are good … until they’re not. Many of the things that commonly give us pleasure can also be used in risky or harmful ways.
When pleasure becomes a problem
Dependence, addiction, bingeing and compulsive consumption can be thought of as risky or harmful uses of otherwise pleasurable experiences, like using alcohol and other drugs, doing exercise and having sex.
It can be difficult to pin down the point at which a previously pleasurable behaviour becomes problematic. But, somewhere between enjoying an occasional beer and needing a drink before getting out of bed each morning, we’ve passed the tipping point.
At this stage though, pleasure is no longer the motivation, nor the result, of the behaviour. The uncontrollable “hunger” has wiped the pleasure away and the best we can hope for is relief. Without pleasure, the behaviour is no longer a hedonic one.
So, when we need to make the mortgage or rent and keep our complex lives on track, what might a modern hedonist’s life look like?
A practical definition might be someone who tries to maximise the everyday pleasures while still balancing other concerns. I’ll call this a kind of “rational hedonism”. In fact, Epicurus emphasised a simple, harmonious life without the pursuit of riches or glory.
Maximising pleasure, unlike with debauchery or addiction, need not take the form of more, bigger, better. Instead, we savour everyday pleasures. We relish them while they’re happening, using all our senses and attention, actively anticipate them, and reflect on them in an immersive way.
So, if my morning coffee gives me pleasure, I might pause and relish it while I drink it: inhale the fragrance of it fully and focus on the nuanced warm, smoky, bitter deliciousness of it. I should fully attend to the warmth of it in my hands, to the feeling of it in my mouth, and to the cascade of sensations and flavours it delivers.
Not only that, in the morning, before my coffee, I can anticipate it. I can think how lovely it will be. And later, as I go about my day, I can pause and think about that coffee, about just how warm and good it was, how it smelled and tasted.
In other words, I can immerse myself in these moments, in the anticipation, in the drinking itself, and in the remembering, and bring all my attention to them.
This kind of savouring results in a totally different, and richer, experience than if I absent-mindedly gulp down the coffee while dodging traffic and talking on the phone.
Why Small Pleasures are a Big Deal discusses how to appreciate the everyday hedonistic pleasures of life, like pleasing textures or smells, without having to spend money on expensive items or experiences.
The act of savouring intensifies the pleasure we extract from simple things and delivers greater satisfaction from them. One study found that spending a little time savouring the anticipation before eating chocolate led participants to eat less chocolate overall.
And attention seems to be key to the link between pleasurable feelings and well-being.
How do we benefit from hedonism?
A state of pleasure is linked with reducing stress. So when we feel pleasure, our sympathetic nervous system – that fight or flight response we experience when we feel threatened – is calmed. First of all, the stimulus arouses us, then if we appraise the situation as safe, we have “stress-terminating responses”, which we experience as relaxation or stress relief.
One study of school children showed focusing on pleasurable daily events, in this case recording them in a diary, reduced depressive symptoms, and the effect was maintained three months later.
Focusing on the pleasurable aspects of healthy foods can also be a more effective way to eat more of them than focusing on how “healthy” they are. Similar approaches are likely to be effective with exercise and other behaviours associated with health benefits.
What we know about the benefits of this kind of rational hedonism is likely to grow from here. We have only just begun to explore the therapeutic value of shifting focus to fully attend to and maximise pleasure.
We do know that interventions encouraging individuals to focus on pleasurable experiences are associated with increased self-reported well-being.
And savouring can be taught. One study, looked at the effects of an eight week program promoting savouring for a group of community dwelling adults aged 60 and above. The program reduced depression scores, physical symptoms and sleep problems, and increased psychological well-being and satisfaction with life.
In the meantime, we should defiantly shake off the idea that pleasure is slightly shameful or frivolous and become early adopters of this rational kind of hedonism. We can think of Epicurus, and intentionally savour the simple pleasures we have learned to overlook.
Read other articles in our hedonism and health series:
Makeup is an everyday item for many people and non-negotiable for some. Is it bad for our skin? As always, the answer is not clear-cut and depends on the individual, their skin type, and the products they use.
With an overwhelming choice of cosmetic products available, most people don’t even know where to start with makeup. Organic? Natural? Fragrance free? Hypoallergenic? Non-comedogenic? Paraben free? What does this all mean, and are they any better?
The term makeup generally describes the group of cosmetics that are used for beautification. Other cosmetics include products that are used to cleanse, treat or protect the skin and hair. These days, though, we commonly see all-in-one products, such as BB or CC creams, which combine makeup for coverage together with other ingredients to provide sun protection and skin benefits. Reducing the total number of products can be helpful for those with problematic skin, but may complicate things for some.
What does makeup do to our skin?
While in most cases makeup is harmless, certain products may cause problems for some individuals. It’s very important to use makeup and cosmetics that are suitable for your skin type or skin condition.
Skin types are broadly classified into four groups:
• oily – excess oil production, large pores, blackheads and acne prone
• sensitive – tight, stinging, intolerant to many products and prone to redness
• dry – dull, rough or flaky and prone to itchiness
• normal/combination – may be oily in the T-zone (forehead, nose and chin) but problem-free elsewhere
Although most people have a good idea of their basic skin type, they may fail to recognise the existence of an underlying skin disorder. Conditions such as eczema, contact dermatitis, rosacea and sun damage may cause inflammation and disruption of the skin barrier.
Inflammation causes itchiness or tenderness, redness, lumps and bumps, while barrier disruption results in tight, sensitive, dry and easily-irritated skin. These symptoms can be identical to those caused by reactions to cosmetics, and therefore should be considered before assuming makeup to be the cause. Conversely, an ongoing reaction to products being applied to the skin may explain why the skin is not responding to regular treatment.
Skin irritations can cause itchy, scaly red rashes. from www.shutterstock.com
Skin problems caused by cosmetics
Acne cosmetica is a form of acne triggered by the use of certain cosmetic products. It is linked to certain ingredients that cause comedone formation (a blockage in the pore) and typically presents as small rash-like bumpy pimples. A common misconception is that the makeup physically blocks the pore, whereas actually the block is made of dead skin cells.
Mild inflammation results in excess skin turnover and clogging of the pore, with mineral oils being the most common culprit. It’s not always possible to determine makeup is the cause simply from the ingredient list, as it may be influenced by formulation, quantity and delivery methods.
Irritant dermatitis accounts for the majority of reactions to makeup and other cosmetic products. It can occur in anyone but is more likely in those with pre-existing sensitive skin or in those with underlying barrier disruption caused by a condition like eczema or rosacea. It typically causes an itchy, scaly red rash but can even blister or weep. Symptoms can occur immediately but may take weeks or even months to develop with weaker irritants, making it difficult to identify the cause.
Allergic contact dermatitis occurs when a person has become sensitised to an ingredient that has been applied to the skin. A red, itchy rash sometimes associated with swelling or blisters develops 12-48 hours after exposure, and may become chronic with ongoing use. The allergen can be very difficult to identify, because in some cases the product is used for months or years before sensitisation occurs.
People put many different products on their face, isolating a cause of irritation can be tricky. from www.shutterstock.com
Are there ingredients we should avoid?
Fragrances and preservatives are the most common cause of contact allergy resulting from cosmetics. There are over 5,000 different fragrances used in skin care products, many of which are natural plant extracts and essential oils.
Other common allergens include preservatives, lanolin, coconut diethanolamide (a foaming agent) and sunscreen agents. Preservatives, such as parabens, formaldehyde and Quaternium-15 are required in all liquid products to stabilise them and prevent the growth of microbes. A common misconception is that natural and organic ingredients will not cause allergy or irritation, but in prone individuals these can in fact be quite problematic.
Unless you have a known allergy or sensitivity, there are no specific ingredients that everyone should avoid. But looking for hypoallergenic, fragrance-free and non-comedogenic products is wise. Those with an oily skin type or a history of acne should also limit oil-based cosmetics.
Those with a sensitive or dry skin type, an underlying inflammatory skin condition or history of contact allergy should try to avoid irritants and potential allergens. Foaming agents, astringent products (such as toners that remove oils), scrubs and acids (such as alpha hydroxy acids used in acne and anti-ageing) tend to be irritating. Hypoallergenic formulations and those targeting sensitive skin are a good choice.
What should I do if I think I might have a reaction?
If you develop a new rash or skin irritation, the first thing to do is to try to confirm the diagnosis. If you suspect you are reacting to one of your cosmetics but not sure which, then ideally you need to stop using all your current products in the problem area. You should try to simplify your daily routine, choosing products that have been specifically formulated for sensitive and allergic skin.
If the problem settles, you can reintroduce your cosmetics one at a time to see whether you can identify the culprit. It’s a good idea to test each one in a small localised area on the neck or face for a week or two before using it all over the face. This process is known as a “repeat open application test”.
If you can’t get to the bottom of it or find cosmetics that don’t irritate your skin, you may need to seek professional help to rule out other skin conditions and formally test for allergies if warranted.
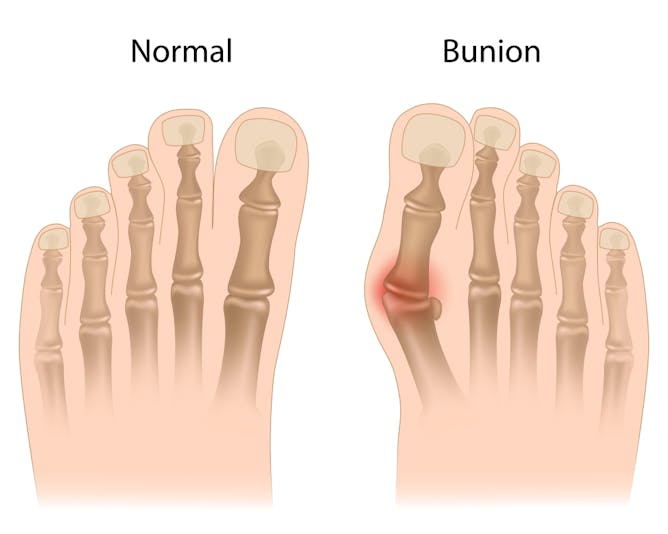
While most people don’t like the sight of bunions, they’re much more than a cosmetic issue. A bunion can cause pain and impact physical function, as well as affecting general health, mental health and social function. Limitations on what footwear can be comfortably worn due to bunions reduces social activities and physical activities.
Scientifically named hallux valgus, a bunion is an enlargement of the inner portion of the joint at the base of the big toe. The enlargement is due to a misalignment of the big toe joint and, in some cases, there is additional bone growth caused by inflammation. The misalignment causes the big toe to point outward towards the other smaller toes.
Bunion can also occur in the fifth toe. This is called a bunionette, or ‘tailor’s bunion’. from www.shutterstock.com
What are the symptoms?
Symptoms can include the joint becoming inflamed with redness, tenderness, and pain. This is due to a small fluid-filled sac called the bursa, which is adjacent to the joint, also becoming inflamed. This is called bursitis.
A deeper joint pain may occur in later stages of the deformity if localised arthritis develops. Over time, the deformity will increase, although the symptoms may not increase.
The pain of bunions and the difficulty finding comfortable footwear impacts on people’s ability to exercise, resulting in reduced physical and mental health. There are also effects on self-image, with patients being uncomfortable with others seeing their feet.
Who is affected?
A recent Australian study found a surprising 36% of participants had this condition, with women and older people more likely to be affected.
What are the causes?
There are a few factors that can lead to bunions including a genetic component. They are caused by faulty foot structures such as having flat feet, excessively flexible ligaments, or abnormal bone structures that lead to the development of bunions.
The Framingham Foot Study found bunions and lesser toe deformities are often inherited in white men and women of European descent.
Shoes also play a significant part, including shoes that are too narrow or wearing high heels for prolonged periods, hence women being over-represented.
Wearing shoes that are too narrow can cause bunions. from www.shutterstock.com
Do bunions need to be treated?
Not all bunions need to be operated on. Conservative treatment is recommended first and then if this doesn’t alleviate the condition (you are unable to walk more than a few blocks and medication and rest don’t reverse the swelling and pain) you may be advised to have surgery.
The severity of the deformity will dictate the extent of the surgical procedures required. There are a number of surgical techniques currently practised.
Bunionectomy is the removal of the inflamed fluid sac from between the skin and bone. Osteotomy is the repositioning of the metatarsal, the big bone in the toe that’s affected. The surgeon may hold the repositioned bone in place with screws, wires, or a metal plate. In severe cases, an artificial joint will be used to replace the existing badly damaged joint. This procedure is called arthrodesis.
Newer minimally invasive surgical techniques are showing positive results for mild to moderate bunions. The advantages to this approach to osteotomy compared to traditional osteotomy are that healing time is minimised and scarring is decreased. The tissues that cross the big toe joint are not damaged in the newer approach, which means there is no joint stiffness after surgery.
If surgical treatment isn’t advised, there are still things you can do to alleviate the condition.
Choice of footwear: your choice of footwear is important. Shoes that are flat, supportive and give you plenty of width for your toes are the best choice. Orthotics may also ease the condition.
Exercises: a podiatrist can recommend specific exercises to treat your symptoms of bunion. These might include going barefoot around the house as this activates the muscles in your big toe joints.
Medication: anti-inflammatory medication may help, and some people receive steroid injections, such as cortisone. These injections reduce the inflammation, and may relieve pain temporarily. Caution is advised as there are many side effects such as infection and bleeding, especially if used frequently and at high doses.
Maintain a healthy weight: this reduces the pressure on your foot joints.
Padding: use of over-the-counter pads can relieve the pressure on your bunions.
What should I do for my bunion?
The best way to find the right treatment for you is to ask your general practitioner or a podiatrist for their advice. The information in this article is general in nature, and your specific case will have to be examined.
Intermittent fasting is currently all the rage. But don’t be fooled: it’s much more than just the latest fad. Recent studies of this kind of fasting – with restricted eating part of the time, but not all of the time – have produced a number of successes, but the latest involving diabetes might be the most impressive yet.
The idea of intermittent fasting arose after scientists were wowed by the effects of constant calorie restriction. A number of studies in many different animals have shown that restricted eating throughout adulthood leads to dramatic improvements in lifespan and general health.
The reasons for these improvements aren’t yet clear. Part of it seems to be that going without food gives cells in the body a much needed break to perform maintenance and repair. But the lack of food also forces cells to resort to alternative sources of energy. Some of these, such as ketones – molecules created in the liver from recycled fat – appear to be beneficial.
‘Fasting’ without fasting
The problem is that constant calorie restriction isn’t practical: it’s easy for scientists to impose upon lab animals, but hard for humans to impose upon themselves in the real world. Fortunately, we’ve learned that constant calorie restriction isn’t really necessary. Intermittent fasting seems to have many of the same benefits.
There are two main types of intermittent fasting. One type, known as “time restricted feeding”, requires eating only during a few hours of the day – say between 10am and 6pm. This approach gives the body a long break from food each night, and also reinforces beneficial circadian rhythms.
The other type of intermittent fasting – made popular by the 5:2 diet – is known as “periodic fasting”. This approach involves alternating between long periods of unrestricted eating and short periods of eating very little (five days of eating normally, two days of eating restricted calories).
It isn’t yet clear whether one type of intermittent fasting is better than the other. But the data so far suggest that both types can work.
Tackling diabetes in mice and men
The recent studies of the effects of intermittent fasting on diabetes have focused on periodic fasting in particular. As a first step, researchers led by Valter Longo at the University of Southern California, began by testing whether periodic fasting could cure diabetes in mice. They used mutant mice that lack the fat hormone leptin to regulate their food intake. These mice constantly overeat and become obese and diabetic in early adulthood.
The researchers found that after just a few months of periodic fasting – alternating seven unrestricted eating days with four restricted days – the diabetes was cured. This is an amazing result. But what’s even more amazing is the reason behind it.
The mice lost weight during the periodic fasting, which helped of course. But that wasn’t the whole story. Periodic fasting actually solved the problem directly at one of its sources: the pancreas.
Diabetes is a disease characterised by excess blood “sugar”, which really means excess blood glucose. It’s largely an insulin problem. Normally, insulin causes cells in the body to take in glucose from the blood. But with diabetes, glucose stays in the blood because cells no longer take it in. This is partly because many cells lose their sensitivity to insulin, but also because the pancreas stops making it.
Glucose meter, healthy lifestyles and nutrition. ratmaner/shutterstock
It turns out that the periodic fasting made the pancreas start producing insulin again. The days of restricted eating gave the pancreas a break that allowed it to remove and recycle many of its cells. Then, when the mice started eating again, new cells that were capable of producing insulin emerged.
So the pancreas actually shrunk during the four restricted eating days, and regrew during the seven unrestricted eating days. After several such cycles of shrinking, recycling, and regrowing, the pancreas was nearly as good as new.
The big question, of course, it whether intermittent fasting will have the same effects in humans. The answer is not yet clear, but the initial indications from a recently published phase two clinical trial, again led by Longo, are promising.
In this study, 100 people went through a series of 30-day cycles of periodic fasting, each with 25 days of unrestricted eating and five days of restricted eating. After only three cycles, those subjects who started the trial with high blood sugar saw big improvements. And, importantly, none of the subjects in the trial experienced any harmful effects.
So the evidence in support of intermittent fasting keeps growing. Does that mean that we should all be doing it? Not necessarily.
Intermittent fasting seems to be most beneficial for those who are already overweight and unhealthy. While it does also seem to have some benefits for lean and healthy lab animals, it’s not yet clear whether the same is true for humans.
A much larger phase three trial of intermittent fasting in humans that will clarify a lot of things is set to begin soon. The results will no doubt be very exciting.
An Australian woman with a genetic disorder died from consuming too many protein supplements, it was recently reported. The woman in question, Meegan Hefford, a 25-year-old bodybuilder, suffered from a rare, undiagnosed disorder that caused a fatal build-up of ammonia in her body (ammonia is produced when the body breaks down protein). This raises the question: are exercise supplements safe?
In healthy people, most commonly used supplements intended to enhance the body – often referred to in the scientific literature as “nutraceuticals” or “functional foods” – are harmless. Nonetheless, there are rare cases where underlying health conditions or excessive consumption could cause ill health.
By far the most common supplement taken by gym goers are those containing amino acids in the form of protein, protein hydrolysates (such as whey protein), or individual branched chain amino acids (BCAA), containing leucine, isoleucine and valine. People take these supplements to support muscle building on the premise that amino acids are the building blocks of muscle tissue. Aside from the rare genetic disorder suffered by Meegan Hefford, are there any dangers to consuming these protein supplements?
There are a number of other very rare genetic disorders where handling of certain amino acids is compromised. For example, maple syrup urine disease (MSUD) leads to a toxic build-up of the BCAA making their over consumption dangerous. Nonetheless, sufferers of MSUD are typically diagnosed at an early age, so this is unlikely to manifest through excessive protein intake in adulthood.
As well as genetic disorders of amino acid handling, people with kidney disease are often told to avoid high protein diets, since excess intake can strain failing kidneys. It is this that led to the premise that high protein diets and, by extension, protein supplements are “bad for the kidneys”.
But this has now largely been debunked, since athletes consuming nearly 3g per kilogram of bodyweight per day (about three-and-a-half times the recommended daily allowance of 0.8g/kg/day) and healthy adults consuming up to 1.25g/kg/day of leucine show very few negative health effects, at least in the medium term. So, apart from in extremely rare cases, taking protein supplements is generally safe.
L-carnitine and creatine
While too numerous to mention, there are a wealth of supplements being consumed by gym goers, with the aim of enhancing muscle mass, reducing fat and increasing performance. Let’s have a look at their safety.
Both L-carnitine and creatine are naturally occurring compounds taken to improve muscle mass, performance or weight loss. (Red meat is particularly rich in these substances.) As with most supplements, these supplements have been subject to many investigations as to their safety. To date, there is minimal evidence that they are harmful to humans, despite early claims of potential liver or kidney damage, muscle cramps or electrolyte imbalances. Also, there are no known underlying diseases which could make them dangerous.
Conjugated linoleic acids (CLA) are another popular supplement. CLA is a specific type of fat that is associated with decreases in fat mass and increases in muscle mass. While generally thought to be safe, there is data from animal models and in humans suggesting their consumption can lead to unfavourable changes in the blood, namely increases in low density lipoproteins (“bad fats”). As is always the case, long-term data from controlled trials is unavailable, so there will always be an element of doubt over their safety.
Vitamin E and resveratrol
But there are other considerations surrounding potentially harmful effects of supplements. A recent example of this are antioxidant supplements, such as vitamin E and reseveratrol. Indeed, while early work purported that these supplements could enhance exercise performance, it later became apparent that, if anything, they could work against the beneficial effects of exercise.
Contamination
Also, rather than the nutrient supplemented being harmful itself, there may be other contaminating compounds within the supplement, unknown to the consumer, that could potentially cause harm.
We often hear news stories about failed drug tests in sport being caused by “contaminated supplements”. Whether this is true or not, there remains real and troubling evidence of contamination within dietary supplements by a number of different controlled substances. Indeed, with control over their production lacking in pharmaceutical rigour, there may be unknown dangers in supplements, particularly those purchased online. A recent case from the US highlights these dangers where a number of people suffered severe acute hepatitis and fulminant liver failure after consuming the same dietary supplement, OxyELITE Pro.
So, while there are few risks to taking supplements (or at least a lack of evidence that they are harmful), it should be remembered that some supplements could negatively affect what people are trying to achieve. Or they could be contaminated to make them appear like “wonder supplements”.
Also, the true efficacy of many emerging supplements is lacking – often being more based on theory and marketing than reproducible science. That being said, a small number of supplements do have proven beneficial effects alongside exercise and moreover many of these have translated into proven clinical benefits .
Going back to protein supplements, yes, they can enhance muscle-mass with exercise, though the effect is small, and supplements could easily be replaced by changes to diet.
About 10% of us (including 20% of people over 60 and 50% of people over 70) suffer from fungal nail infections. So why do we get them, and does it matter?
Technically called “onychomycosis”, fungal infection of the nail plate (the hard outer nail) or nail bed (that lies under the hard nail) will most often appear as yellowish, white, black or green discolouration of the nail. The infected nail may also appear thickened or brittle. In severe cases, from long-term infection (where all the tissues of the nail have been infected), the infected nail may break up and fall off.
Fungal nail infections can be difficult to cure, and they typically don’t go away without antifungal treatment. The fungus can spread to other areas of the hands or feet, and can be mild with purely cosmetic implications, or more severe with pain, low self-esteem and embarrassment due to disfigurement.
Toenails are more often affected than fingernails, possibly because they’re larger, slower to grow, suffer pressure from footwear, often have poorer hygiene, and are often in a closed environment (shoes) where fungi can grow.
Although fungal nail infections are not life-threatening, they’re an important health problem because of their high prevalence and poor response to therapy.
Fungal nail infections are thought to have become more prevalent during the 20th century thanks to people migration, longer life expectancy, increasing numbers of people with compromised immune systems (such as HIV sufferers), use of stifling foot wear and locker rooms in the gym.
Causes and symptoms
Fungal nail infections are caused by different types of fungi, yeasts (such as Candida) and moulds. Fingernail fungal infections are typically caused by yeast fungi, especially Candida.
Fungal infection of the fingernails is less common than toenails. from www.shutterstock.com
Fungal nail infections are more common among people who are of lower socioeconomic background, older, male, diabetic, obese, immune deficient (such as HIV or cancer), lacking personal hygiene, and environmental factors such as fungal contamination of swimming pools, public toilets and communal bathing facilities.
One of the problems with treating fungal nail infections is the fungus that causes it is difficult – if not impossible – to eliminate from the environment. These fungi thrive in warm, moist environments that you typically find in gyms, swimming pools, bathrooms, socks of unnatural fibres and enclosed shoes.
Because fungal spores can remain viable for months in these environments, frequent exposure can increase the risk of infection (and re-infection). Fungal spores can be picked up in many ways – such as wearing shoes that harbour the organism, by walking barefoot in areas where the fungus is prevalent (especially public showers and locker rooms), by wearing wet shoes or socks for long periods, through previous injury to the toe or toenail that opens a path for easy entry of the fungus, or by wearing improperly-fitting shoes.
Fungal infection occurs when the organism invades through an opening in the nail, meaning fungi will usually attack nails that are already damaged. After infection occurs, the growth of the fungi leads to mild inflammation, which causes the nail to thicken and the nail plate to detach from the nail bed. The space underneath the nail can then serve as a reservoir for bacteria and moulds, which can cause the nail to become discoloured.
Diagnosis and treatment
Fungal nail infections and the resultant nail destruction can promote other sources of infection like cellulitis (a bacterial skin infection) and other forms of tinea, and aggravate foot problems resulting from other illnesses such as diabetes. Diagnosis is usually confirmed by looking at nail clippings through a microscope or other tests before starting treatment.
Treatment may not be required if the infection is minor. The severity is judged by looking at the degree of discolouration, nail thickening and pain.
Topical agents such as amorolfine (Loceryl 5% nail lacquer; applied once or twice a week) and ciclopirox (Penlac 8% nail lacquer; applied daily) are usually prescribed for mild forms of the disease, but the treatment periods are long and their efficacy is somewhat limited due to poor nail plate penetration. These medications kill fungi by interfering with their cell membranes, which leads to their death.
For more severe cases, oral antifungal medications might be required. These include fluconazole (an antifungal agent also commonly used to treat thrush), terbinafine (a broad-spectrum antifungal) and griseofulvin (usually used for skin infections). The latter is a very old drug and carries the risk of causing damage to the liver. Terbinafine is most effective and therefore is the preferred oral treatment. A 12-week course cures 70-80% of cases by causing the fungi’s cells to leak and die. It can, however, cause gastrointestinal side effects and depression.
Most nails with extensive fungal infection may still look disfigured even after 12 weeks of treatment, as the nail plate grows slowly and it takes about nine months to grow out fully. Even once the fungus is successfully eradicated, there may be long-term effects on the appearance of the nail.
When you go to your doctor, marking a line on the nail with a scalpel blade at the base of where the fungus starts is helpful for treatment follow-up. The patient can follow the marking as the nail grows out. If the newly grown-out nail is growing out discoloured, further treatment is required.
Onychomycosis patients may need to learn new, healthier habits to stop the fungus growing back. These could include protecting toes from sources of infection, wearing correctly fitting footwear, laundering socks in hot water with disinfectant, wearing protective footwear at the pool and gym, keeping nails short, using open-toed footwear and wearing shoes made of breathable material.
Kavya E.Baby, Medical Registrar (basic physician trainee) at Canberra hospital, contributed to this article.